Nail Haematoma: Cuticle and Subungual Types
Author: Radina Ignatova, Professional Nail Expert | Last Updated: February 2026
Quick Summary
Nail haematoma refers to blood pooled under the skin from burst capillaries, occurring in two distinct locations: cuticle haematoma (proximal nail fold) and subungual haematoma (under the nail plate). Both types are typically caused by trauma or injury.
Both cuticle and nail haematomas represent absolute contraindications for all nail services including e-file work, manual cuticle manipulation, and product application. Professional nail technicians must recognise visible bruising, swelling, tenderness, or recent trauma as warning signs requiring immediate service suspension. Continuing with any nail service on damaged tissue delays healing, increases infection risk, and can cause permanent nail matrix damage.
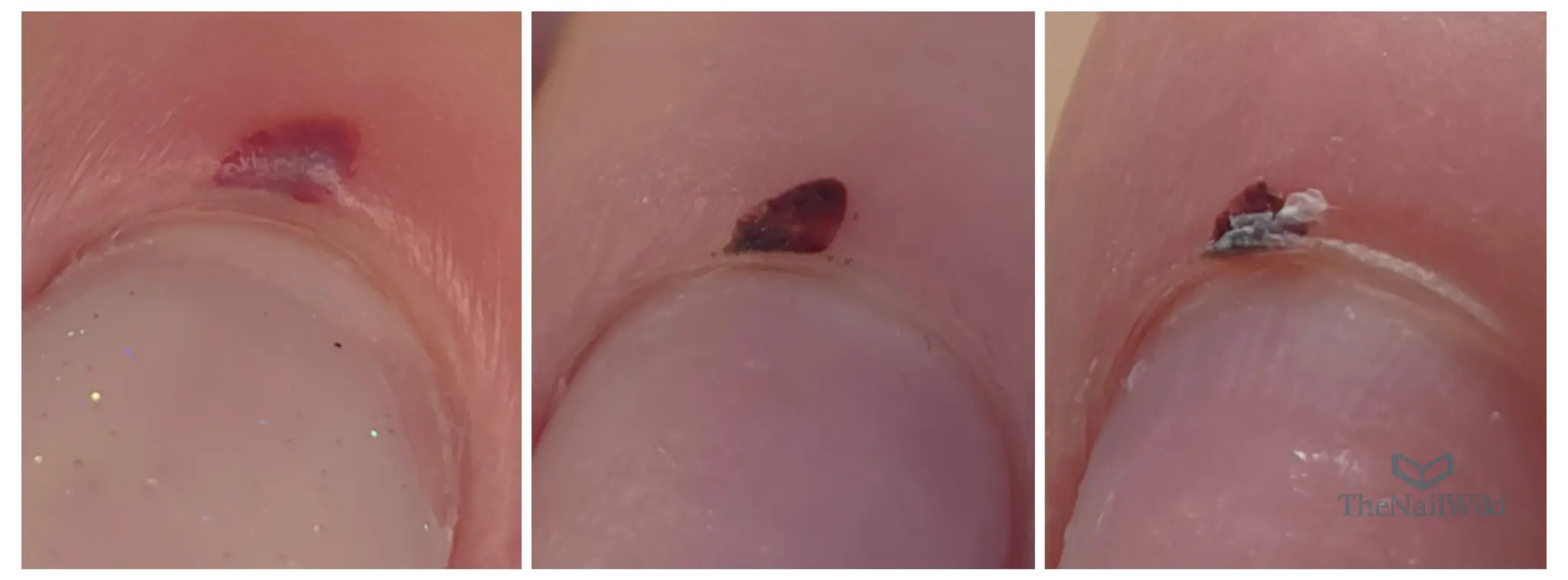
Professional demonstration: Real example of cuticle haematoma and why continuing any nail service would cause genuine harm. This video shows actual salon decision-making for client safety.
Contents
Professional nail services require continuous assessment of tissue health and client suitability. Whilst educational content often demonstrates techniques under ideal conditions, real salon work involves clients presenting with various tissue compromises including bruising, inflammation, and recent trauma to both the proximal nail fold (cuticle area) and the nail bed beneath the nail plate.
The ability to recognise contraindications and make appropriate professional decisions separates trained technicians from those operating outside safe practice parameters. Nail haematomas—whether occurring in the cuticle area or beneath the nail plate—represent some of the most commonly encountered contraindications in nail services, yet remain poorly understood in terms of risk assessment and professional response.
Definition and Pathophysiology
A haematoma is an accumulation of blood outside blood vessels, caused by damage to the vessel wall. In the context of the proximal nail fold (cuticle area), haematomas typically result from blunt trauma that ruptures capillaries within the dermis.
Tissue Response to Trauma
When trauma occurs to the cuticle area, several physiological processes begin:
- Capillary rupture: Small blood vessels break, releasing blood into surrounding tissue
- Blood pooling: Haemoglobin accumulates in extravascular space, creating visible discolouration
- Inflammatory response: The body initiates healing through increased blood flow and cellular activity
- Tissue compromise: The affected area becomes more vulnerable to further damage and infection
Visible Characteristics
Haematomas present with characteristic colour changes depending on the stage of healing:
- Acute (0-2 days): Red to purple discolouration from fresh blood
- Early healing (3-5 days): Blue to dark purple as haemoglobin breaks down
- Mid-healing (6-10 days): Green to yellow as bilirubin forms
- Late healing (10-14 days): Yellow to brown as reabsorption completes
⚠️ Critical Safety Note
Absence of pain does not indicate safety to proceed with nail services. Damaged tissue beneath intact skin remains vulnerable to further trauma, infection, and delayed healing regardless of the client’s pain threshold or subjective comfort level.
Types of Nail Haematoma
Nail haematomas occur in two distinct anatomical locations, each with specific characteristics, appearance, and professional implications. Understanding the difference between these types is essential for accurate assessment and appropriate response.
Cuticle Haematoma (Proximal Nail Fold)
A cuticle haematoma occurs in the soft tissue of the proximal nail fold—the area commonly referred to as the “cuticle.” Blood accumulates in the dermal and subdermal layers of this tissue following trauma.
Characteristics of cuticle haematomas:
- Location: Within the soft tissue surrounding the base of the nail plate, typically on the dorsal (top) surface of the proximal nail fold
- Appearance: Red to purple discolouration visible through or beneath the skin surface, progressing through colour stages during healing
- Texture changes: May present with swelling, puffiness, or skin flaking during late-stage healing as shown in the progression images
- Common causes: Trauma from impacts (door catches, hitting against objects), overly aggressive cuticle work, repeated friction, or crushing injuries
- Healing duration: Typically 7-14 days for minor haematomas; larger or deeper bruising may require 4-5 weeks as demonstrated in the images, particularly when tissue damage is extensive
- Service implications: All cuticle work contraindicated including e-file, manual nippers, pushers, and any product application requiring proximal nail fold contact
Subungual Haematoma (Under Nail Plate)
A subungual haematoma occurs beneath the nail plate within the nail bed. Blood becomes trapped between the nail plate and the underlying nail bed tissue, creating characteristic dark discolouration visible through the translucent nail plate.

Characteristics of subungual haematomas:
- Location: Between the nail plate and nail bed, typically visible as discolouration through the nail plate
- Appearance: Dark purple, brown, or black discolouration beneath the nail plate that does not blanch (turn white) when pressure is applied
- Progression: Does not change colour like tissue haematomas; instead, the discolouration remains until the affected nail plate grows out completely
- Common causes: Direct trauma to the nail (dropping objects on the nail, crushing injuries, stubbing toes, repetitive pressure from poorly fitted shoes)
- Pain presentation: Often acutely painful immediately after injury due to blood pressure beneath the rigid nail plate; may cause throbbing sensation
- Medical considerations: Large subungual haematomas covering more than 25-50% of the nail bed may require medical evaluation for nail plate removal to prevent infection and assess underlying damage
- Healing duration: Determined by nail growth rate; discolouration remains until affected nail plate portion grows out completely (typically 3-6 months for fingernails, 9-18 months for toenails)
- Service implications: All nail services contraindicated on affected digit including filing, buffing, cuticle work, and product application until damaged nail plate section has grown out and been removed
Key Differences Between Types
Professional Assessment Priority
Both types of nail haematoma require immediate service suspension. Technicians should document the type, size, location, and appearance in client records. For subungual haematomas covering significant nail bed area, recommend medical evaluation before scheduling future services. Never attempt to file, buff, or otherwise work on nail plates with visible subungual haematomas, as this can worsen underlying tissue damage.
Clinical Recognition
Professional assessment begins with systematic visual and physical examination of all nail areas before commencing any service. Haematomas may be immediately obvious or subtle depending on severity, timing, and individual tissue response. Implementing a comprehensive nail consultation process ensures consistent screening for contraindications including haematomas.
Visual Assessment Criteria
During pre-service consultation, technicians should examine each digit for the following visual indicators:
- Discolouration: Any purple, red, blue, dark, green, or yellow colouring under the skin
- Swelling: Visible puffiness or enlargement compared to unaffected digits
- Asymmetry: Differences in tissue appearance between corresponding fingers
- Skin integrity: Breaks, cuts, or compromised skin over or near the haematoma
- Nail plate changes: Discolouration, lifting, or separation associated with trauma
Physical Assessment Criteria
Gentle palpation provides additional diagnostic information:
- Tenderness: Pain or discomfort when the area is lightly touched
- Heat: Increased temperature indicating active inflammation
- Firmness: Hardness or resistance compared to healthy tissue
- Client reaction: Flinching, withdrawal, or verbal indication of sensitivity
Client History Indicators
Direct questioning during consultation may reveal:
- Recent injury (caught in door, knocked against object, crush injury)
- Awareness of bruising or soreness in the area
- Timeline of trauma (days to weeks prior)
- Previous services that caused discomfort or bleeding
- Use of blood-thinning medications that increase bruising susceptibility
Documentation Standards
All visual and physical findings should be documented in client records, including the specific location, size, colour, and client-reported history. Photographic documentation (with client consent) provides valuable reference for monitoring healing progression between appointments.
Contraindications for Nail Services
The presence of a cuticle haematoma constitutes an absolute contraindication for the affected digit across all nail service types. This restriction is not based on pain tolerance or client preference, but on tissue physiology and infection control principles.
E-File Services
Electric file work presents particular risk to haematoma sites due to:
- Friction heat generation: Even low-speed bits create thermal energy that increases inflammation in compromised tissue
- Mechanical pressure: Contact between rotating bit and skin applies force that can rupture additional capillaries
- Vibration transmission: Tool vibration travels through tissue, potentially disturbing clot formation and healing processes
- Skin breach risk: Damaged tissue has reduced structural integrity and tears more easily under e-file contact
Manual Cuticle Work
Hand tools pose equivalent risks despite lower speeds:
- Cuticle nippers: Cutting compromised tissue increases bleeding risk and creates bacterial entry points
- Cuticle pushers: Pressure against damaged skin can extend bruising and delay healing
- Metal implements: All manual tools apply force to tissue already in a compromised state
- Scraping actions: Even gentle manipulation disturbs healing processes
Product Application Services
Whilst product application may appear less invasive, contraindications persist:
- Nail preparation: Buffing and dehydration steps near haematoma sites risk skin contact and trauma
- Chemical exposure: Primers, bonders, and gel products cause additional irritation if skin barrier is compromised
- Cleanup procedures: Removing excess product around cuticles applies pressure to damaged tissue
- Curing heat: UV/LED lamp heat increases inflammation in actively healing tissue
⚠️ Professional Liability
Working on visibly damaged tissue despite recognised contraindications may void professional insurance coverage. Documented awareness of haematoma presence followed by service provision creates liability exposure if complications develop.
Professional standards require service suspension regardless of client insistence or financial considerations.
Complications from Working on Damaged Tissue
Proceeding with nail services despite haematoma presence creates measurable clinical risks with documented consequences. These complications range from delayed healing to permanent tissue damage.
Extension of Haematoma
Mechanical stress from any nail service tool can rupture additional capillaries in tissue already compromised by existing vascular damage. Small haematomas expand into larger areas of bruising, extending both the visible discolouration and the required healing time. This occurs because damaged blood vessels in the vicinity of the original injury have weakened walls that rupture more easily under pressure.
Delayed Healing Timeline
The body’s healing cascade requires undisturbed tissue to progress efficiently. When nail services interrupt this process:
- Clot disruption: Mechanical action dislodges forming clots, restarting the bleeding cascade
- Inflammatory response prolongation: Additional trauma extends the inflammatory phase beyond normal duration
- Cellular repair interference: Fibroblasts and other repair cells cannot function optimally in actively stressed tissue
- Extended timeline: Haematomas that would resolve in 7-14 days may take 3-4 weeks when repeatedly disturbed
Infection Risk Elevation
Compromised tissue presents reduced resistance to bacterial colonisation. Haematomas specifically increase infection susceptibility through several mechanisms:
- Skin barrier compromise: Even microscopic breaks in skin integrity create bacterial entry points
- Blood as culture medium: Pooled blood provides nutrients supporting bacterial growth if skin is breached
- Reduced immune response: Damaged tissue has impaired local immune function
- Tool contamination risk: Any implement contacting damaged tissue can introduce pathogens
Nail Matrix Damage
Severe or repeated trauma to the proximal nail fold can affect the underlying nail matrix, the tissue responsible for nail plate production. Consequences include:
- Permanent ridging: Disrupted matrix cells create longitudinal ridges in emerging nail plate
- Nail dystrophy: Severe matrix damage causes permanent nail deformity
- Growth disruption: Temporary or permanent slowing of nail growth rate
- Colour changes: Matrix trauma can cause permanent nail discolouration
Professional Experience Evidence
Professional observation demonstrates that mechanical stress during the inflammatory healing phase (0-7 days post-injury) significantly increases complication rates and healing duration. Clinical experience shows infection rates increase substantially when damaged tissue is manipulated before healing completes.
Professional Response Protocols
When haematoma is identified during pre-service assessment, technicians have several evidence-based response options. The selected approach depends on haematoma severity, location, and client service requirements.
Complete Digit Exclusion
For significant haematomas or those covering substantial proximal nail fold area, complete service suspension for that digit represents the safest response. This protocol involves:
- No cuticle work of any kind (manual or e-file)
- No nail plate preparation in the proximal area
- No product application if it requires working near the haematoma site
- Documentation of exclusion reason in client records
- Rescheduling of services for that digit after healing
Localised Avoidance Protocol
When haematoma is confined to one side or section of the proximal nail fold, technicians may be able to work around the damaged area whilst maintaining safety standards. This requires:
- Clear demarcation: Identifying precise boundaries of damaged tissue
- Tool modification: Using smaller bits or implementing manual work only in safe zones
- Pressure reduction: Eliminating all contact with or near the haematoma site
- Product placement precision: Ensuring no gel or product contacts damaged tissue
- Conservative approach: Accepting incomplete cuticle work rather than risking trauma
Deferred Service Approach
For clients requesting complete services on all digits, deferral of the affected digit until healing completes presents the optimal solution:
- Complete services on unaffected nine digits during current appointment
- Schedule follow-up appointment 7-14 days later for affected digit
- Provide no-charge or reduced-rate completion service after healing
- Document arrangement in client records
- Reassess healing status at follow-up before proceeding
⚠️ Client Pressure Response
Clients may request technicians proceed despite haematoma presence, citing pain tolerance, time constraints, or aesthetic preferences. Professional standards require refusal of such requests.
No client request supersedes tissue safety requirements. Technicians should explain that proceeding would represent unprofessional practice that could harm the client and violate professional standards.
Healing Timeline and Tissue Recovery
Understanding normal haematoma resolution timelines enables technicians to make informed decisions about when tissue has recovered sufficiently for safe service provision.
Standard Healing Progression
Uncomplicated haematomas follow a predictable healing timeline:
- Days 0-3: Acute phase with visible red-purple bruising and potential swelling
- Days 4-7: Colour change to blue-purple as haemoglobin breakdown begins
- Days 8-10: Green-yellow discolouration as biliverdin and bilirubin form
- Days 11-14: Yellow-brown fading as tissue reabsorbs breakdown products
- Days 14+: Return to normal tissue colour and texture
Factors Affecting Healing Duration
Several variables influence individual healing timelines:
- Haematoma size: Larger accumulations require extended reabsorption periods
- Tissue depth: Deeper haematomas persist longer than superficial ones
- Age: Older clients typically experience slower healing rates
- Medication: Blood thinners, corticosteroids, and immunosuppressants extend healing time
- Health status: Diabetes, vascular disease, and immune disorders slow tissue recovery
- Repeated trauma: Additional injury to healing tissue restarts the healing cascade
Service Resumption Criteria
Technicians should verify all of the following before resuming services on previously affected digits:
- Complete resolution of visible discolouration
- Absence of swelling or tissue abnormality
- No tenderness on palpation
- Normal tissue temperature (no residual inflammation)
- Client reports no residual soreness or sensitivity
- Minimum 7 days elapsed since injury (14 days preferred for complete healing)
Conservative Approach Recommended
When in doubt about healing status, err towards postponing services. Tissue that appears healed visually may retain subclinical inflammation or vulnerability. An additional week’s delay has minimal impact on the client but eliminates risk of complication from premature service resumption.
Client Communication
Professional communication about service suspension due to haematoma requires balancing client education, professional authority, and empathetic service delivery.
Recommended Communication Framework
Effective client communication includes several key elements:
- Observation statement: “I can see you have some bruising under the skin on this finger.”
- Safety explanation: “Working on it with any tools would delay healing and could make it worse.”
- Professional decision: “I am going to leave this one and focus on the others.”
- Timeline guidance: “It should be healed enough for next time.”
- Alternative offering: “We can complete this finger at your next appointment when it has healed.”
Addressing Client Concerns
Common client questions and professional responses:
Client: “It does not hurt, can you not just be careful?”
Response: “The tissue underneath is damaged even though the surface looks fine. Any work I do would cause additional damage that you would notice after you leave. I need to prioritise your nail health over completing the service today.”
Client: “How long until I can have it done?”
Response: “These typically heal in 7 to 14 days. I can see you at your next appointment and assess whether it is ready. If it has not fully healed, we will wait a bit longer.”
Client: “My previous technician always worked on them anyway.”
Response: “I understand different technicians have different approaches. However, my training and professional standards require me to stop when I see damaged tissue. This protects both you and my professional licence.”
Professional Boundaries
Technicians should maintain firm professional boundaries regardless of client pressure:
- Never proceed with services on compromised tissue regardless of client requests
- Do not offer reduced-quality work as a compromise
- Maintain calm, professional tone even if client becomes upset
- Document refusal and reasoning in client records
- Recognise that clients who cannot respect professional boundaries may not be suitable long-term clients
Frequently Asked Questions
What is the difference between a cuticle haematoma and a subungual haematoma?
A cuticle haematoma occurs in the soft tissue of the proximal nail fold (cuticle area) and heals through tissue reabsorption over 7 days to 5 weeks depending on severity. A subungual haematoma occurs beneath the nail plate in the nail bed and appears as dark discolouration visible through the nail. Subungual haematomas do not reabsorb; instead, the affected nail portion must grow out completely, which takes 3-6 months for fingernails or 9-18 months for toenails. Both types require complete service suspension until healed.
Can I use manual tools instead of an e-file on a haematoma?
No. The contraindication applies to all implements regardless of whether they are powered or manual. Cuticle nippers, pushers, metal implements, and buffers all create pressure and friction that can worsen the haematoma, delay healing, and increase infection risk. The tissue damage exists regardless of which tool you might use.
How do I explain to clients why I cannot work on their haematoma?
Use clear, professional language: “I can see you have bruising under the skin on this finger. Working on it would delay healing and could make it worse. I am going to leave this one and focus on the others. It should be healed for next time.” Most clients appreciate honesty and see it as evidence of professional care rather than service refusal.
Can I apply gel polish over a subungual haematoma if the nail plate looks intact?
No. Even though the nail plate surface may appear intact, the underlying nail bed tissue is damaged. Filing, buffing, or applying product to the nail plate can transmit pressure and vibration to the injured nail bed beneath, worsening tissue damage and potentially causing nail plate separation. Additionally, the damaged tissue is at higher risk for infection if any product seeps beneath the nail plate. All services must be suspended until the damaged nail plate section has grown out completely and been removed.
How long does a cuticle haematoma take to heal completely?
Small cuticle haematomas typically resolve within 7 to 14 days in healthy individuals. However, larger or deeper bruising may require 4 to 5 weeks for complete healing, as demonstrated in clinical progression images. Healing time depends on haematoma size, depth, individual health status, age, and whether the area remains undisturbed. Working on the haematoma during the healing phase significantly extends this timeline and increases complication risk.
What other conditions require me to stop nail services?
Do not work on tissue showing: active infection (pus, extreme redness, heat), open wounds or cuts, severe inflammation, skin conditions (psoriasis, eczema, dermatitis), extremely thin or damaged nail plates, warts, fungal infections, or if the client uses blood-thinning medications without physician clearance. Any visible tissue compromise requires assessment and potential service suspension.
Will clients be upset if I refuse to work on one finger?
Professional clients appreciate safety-focused decision-making. When you explain the reasoning clearly and offer alternative solutions (completing the digit after healing), most clients respect your judgment. Clients who become upset about safety protocols are typically not suitable for long-term professional relationships. Your reputation benefits from prioritising client health over immediate service completion.
Can I apply gel polish to the nail plate whilst avoiding the haematoma area?
This depends on haematoma location and severity. If the haematoma is confined to one side and you can complete all preparation and application steps without any contact with or pressure near the damaged tissue, limited product application may be possible. However, if any step requires working near the haematoma, suspend the entire service for that digit. When in doubt, exclude the digit completely.
What if the client insists the haematoma does not hurt?
Absence of pain does not indicate safety to proceed. Damaged tissue beneath intact skin remains vulnerable regardless of pain levels. Some individuals have high pain thresholds or damaged tissue may not produce strong pain signals. Professional standards require stopping based on tissue appearance and damage evidence, not client pain tolerance. Explain that proceeding would cause harm even if it does not hurt immediately.
Related Articles
About This Article: This educational content is based on professional nail industry experience, established contraindication protocols, and standard safety practices for nail services. The information provided represents professional guidance for nail technicians and is not intended as medical advice. For specific medical conditions or concerns, clients should consult qualified healthcare professionals.
About the Author

Radina Ignatova
Professional Nail Expert since 2014 | International Nail Educator | Founder of TheNailWiki and Artistic Touch Nail Training Academy
Radina Ignatova is a Professional Nail Expert since 2014 and an International Nail Educator specialising in dual forms, gel systems, polygel application, advanced nail structure, E-File techniques and professional salon safety.
She founded TheNailWiki to provide clear, safety-led nail education accessible to everyone, and Artistic Touch Nail Training Academy to deliver structured professional online nail courses.
Her teaching philosophy is centred on honest education — demonstrating real salon challenges, practical corrections and performance-based techniques rather than presenting only polished results.
Based in Scotland, UK, Radina contributes to advancing professional standards within the nail industry through structured educational resources and technical training. Read full bio.
About TheNailWiki: TheNailWiki is an independent educational platform dedicated to providing accurate, safety-led and professionally informed nail care information to professionals and enthusiasts worldwide. All content is created by qualified nail industry professionals and reviewed for technical accuracy.
Our mission is to provide accurate, safety-focused and professionally informed nail education that is accessible to everyone. For structured professional training, advanced masterclasses, and specialist technique courses, visit Artistic Touch Nail Training Academy.