Lichen Planus Affecting the Nails: Signs, Risks and Professional Considerations
Author: Radina Ignatova, Professional Nail Expert & International Nail Educator | Last Updated: May 2026
Quick Summary
Lichen planus is a chronic inflammatory condition affecting the skin, mucous membranes, and — in a significant proportion of cases — the nails. When it affects the nail unit, it produces characteristic changes in the nail plate structure and can, in severe or untreated cases, cause permanent and irreversible nail loss.
It is not contagious. For nail professionals, lichen planus affecting the nails is one of the more clinically significant conditions to be aware of — both because of the potential for permanent damage and because early referral can meaningfully affect the outcome for the client.
Contents
What Is Lichen Planus?
Lichen planus is a chronic inflammatory condition of unknown precise cause, thought to involve an abnormal immune response against the body’s own epithelial cells. It most commonly affects the skin — where it presents as itchy, flat-topped, violaceous (purplish) papules — and the mucous membranes of the mouth and genitals. Nail involvement occurs in an estimated 10% of people with lichen planus, though the nails may be the only site affected in some individuals.
The condition can affect any nail, and may affect multiple nails simultaneously. It is not contagious. The cause of nail involvement is direct inflammatory attack on the nail matrix — the structure responsible for producing the nail plate — which is why the resulting nail changes are structural rather than superficial.
How Lichen Planus Affects the Nails
Because lichen planus targets the nail matrix, its primary effects are seen in the nail plate structure — the output of the matrix. The nail bed can also be involved, adding further signs to the clinical picture.
Longitudinal ridging and furrowing
Ridges running the length of the nail — longitudinally — are among the earliest and most characteristic signs of nail lichen planus. In early stages, the ridging may be subtle, resembling normal ageing changes in the nail plate. As the condition progresses, the ridges deepen and multiply, giving the nail plate a corrugated or channelled appearance.
Nail plate thinning
The inflammatory damage to the matrix reduces its capacity to produce a full-thickness nail plate, causing the plate to become progressively thinner. A thinned plate is fragile and prone to splitting, crumbling at the free edge, and breaking under normal daily use.
Onycholysis
Separation of the nail plate from the nail bed — onycholysis — can occur in nail lichen planus as a result of bed involvement by the inflammatory process. The onycholysis in this context is driven by the condition itself rather than by external mechanical factors and will not resolve without treatment of the underlying condition.
Pterygium unguis
Pterygium unguis — the forward migration of the proximal nail fold skin onto the nail plate surface — is a hallmark sign of nail lichen planus and indicates significant scarring of the matrix beneath. The skin creeps forward to fill the space where the nail plate has been lost or destroyed. This is an irreversible change: where pterygium has formed, the nail plate will not regrow. The extent of pterygium formation reflects the extent of permanent matrix damage.

© TheNailWiki
Twenty-nail dystrophy
When all twenty nails are affected — showing uniform roughness, longitudinal ridging, and brittleness — this presentation is known as twenty-nail dystrophy or trachyonychia. While twenty-nail dystrophy has multiple possible causes, lichen planus is one of the most significant among them. The nails appear sandpaper-like in texture and dull in appearance.
The Risk of Permanent Nail Damage
Unlike many nail conditions, lichen planus carries a genuine risk of permanent, irreversible nail loss if left untreated or if treatment is delayed. The inflammatory process directly attacks the nail matrix, causing progressive scarring. Once the matrix is scarred, it cannot regenerate — meaning the nail plate it would have produced is permanently lost.
This is why early referral matters. A client presenting with progressive nail thinning, deepening longitudinal ridges, or pterygium formation affecting one or more nails — particularly if it does not have an obvious mechanical explanation — should be referred for dermatological assessment without delay. The window for preventing permanent loss may be limited.
The severity of outcome varies considerably between individuals. Some people experience mild nail changes that stabilise with treatment. Others experience progressive scarring and partial or complete permanent nail loss on affected digits. Outcomes are generally better when treatment is initiated early, before significant scarring has occurred.
Professional Considerations in the Salon
Fragility requires adapted technique
Nails affected by lichen planus are structurally fragile — thinned, ridged, and prone to splitting. Any mechanical work on or around these nails must be extremely gentle. Aggressive filing, buffing, or cuticle work risks causing further damage to an already-compromised nail plate and the structures beneath it.
Trauma risk and the nail matrix
Because the nail matrix is the primary site of damage in lichen planus, any trauma to the proximal nail area — including the eponychium and proximal fold — carries additional risk. Cuticle work in this zone should be minimal and non-invasive. E-file work near the proximal fold is contraindicated in active disease.
Product application considerations
Whether nail products can be applied to nails affected by lichen planus depends on the individual nail condition. A thinned, fragile nail plate may not provide adequate support for enhancements. Where onycholysis is present, product must not be applied over the separated zone. Colour cosmetic products — gel polish or standard polish — may be appropriate on minimally affected nails, with the caveat that removal must be gentle.
Always obtain informed consent from the client and document the nail condition and any adaptations made before proceeding.
Pterygium — do not attempt removal
Pterygium unguis attached to the nail plate should never be manipulated, lifted, or attempted to be pushed back in the salon. The skin has adhered to the plate due to scarring beneath, and any attempt to separate it risks bleeding, pain, and further trauma to an already-damaged area. This is a clinical finding that requires medical management only.
When to Refer
Given the risk of permanent nail loss, the threshold for referral in potential nail lichen planus should be low. Refer promptly when:
- A client presents with progressive nail thinning, deepening longitudinal ridges, or fragility without a clear mechanical cause
- Pterygium unguis is observed — the forward migration of proximal fold skin onto the nail plate
- Multiple nails are affected simultaneously with similar changes
- The client reports that nails are progressively worsening
- All twenty nails show trachyonychia-type changes (rough, ridged, sandpaper texture)
- Any suspected nail lichen planus without confirmed diagnosis — early dermatological assessment is essential given the irreversibility of late-stage changes
Common Misconceptions
❌ “Longitudinal ridging is just a sign of ageing”
Fine longitudinal ridging does become more common with age, but deep, progressive, or worsening longitudinal ridges — particularly in a younger person or accompanied by thinning and splitting — should not be dismissed as normal ageing. These can be early signs of nail lichen planus and merit investigation.
❌ “The pterygium can be pushed back like a cuticle”
Pterygium unguis in lichen planus is not the same as an overgrown cuticle. It is scar tissue adherent to the nail plate due to permanent matrix damage beneath. Attempting to push it back or manipulate it as you would cuticle tissue risks injury and additional trauma to an already severely compromised nail unit.
❌ “It will improve on its own without treatment”
Lichen planus affecting the nails can progress to permanent nail loss if the inflammatory process continues unchecked. While some cases stabilise, others do not, and the window for preventing permanent damage may close without timely medical intervention. This is not a condition that should be observed and monitored indefinitely without professional medical assessment.
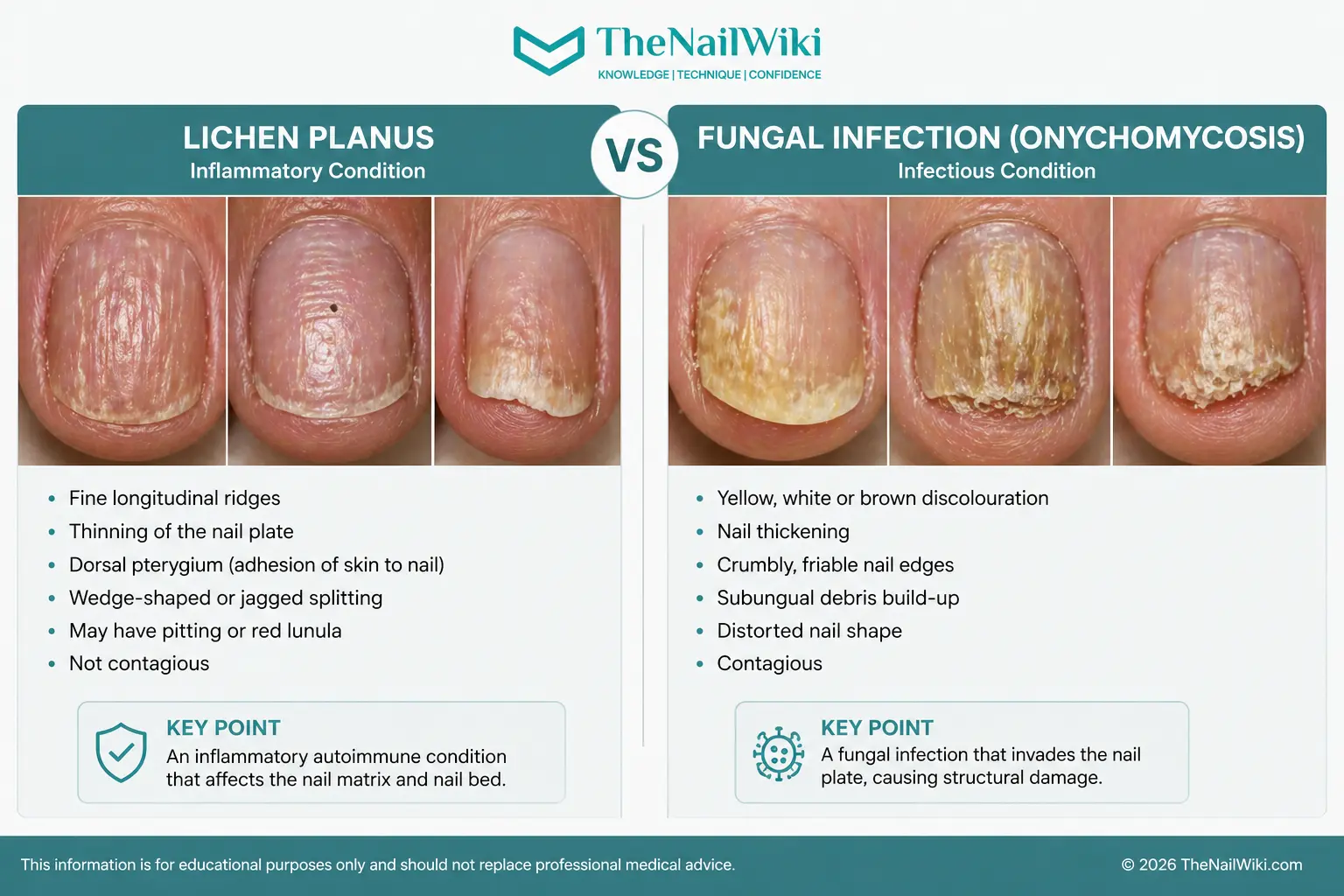
Lichen Planus vs Fungal Infection — Recognising the Difference
One of the most common errors in professional nail assessment is mistaking subungual changes — whether from lichen planus, nail psoriasis, or other conditions — for a fungal nail infection. Subungual hyperkeratosis — the build-up of keratinous debris beneath the nail plate that occurs in lichen planus — can look visually similar to fungal disease. The cause, the behaviour, and the professional decisions that follow are entirely different.
This distinction matters because fungal infection is contagious — it requires refusal of service, referral, and strict hygiene management. Lichen planus is not infectious — it is an autoimmune inflammatory condition. Treating the two the same way leads to either refusing service unnecessarily or, far more dangerously, applying product over an active infection and spreading it through tools to other clients.
© TheNailWiki
The mistake that causes most harm
The most common incorrect assumption is that anything found beneath the nail plate — debris, scale, discolouration — is either product lifting, dirt, or something that can be cleaned out and worked over. This thinking leads directly to two categories of serious error: applying product over an active fungal infection, and using tools on infected nails that then contact other clients without adequate sterilisation.
Recognising that subungual changes have different causes — and that some are not infectious while others are — is not an advanced skill reserved for medical professionals. It is a foundational part of professional nail assessment. A nail technician does not need to diagnose the specific condition. They do need to recognise that something is present that requires assessment before any service decision is made.
Fungal infection — service must not proceed
If fungal nail infection is suspected — crumbly debris, progressive yellow or brown discolouration, spread to adjacent nails, or characteristic odour — do not perform the service. Do not apply product over the affected nail. Refer the client to their GP or podiatrist. Any tools that have contacted the area must go through the full decontamination process before use on any other client.
Lichen planus — service may proceed with adaptation
Lichen planus is not contagious. A service may be appropriate depending on the severity of the nail changes present, the stability of the condition, and whether the nail plate can safely support any product. The service must be adapted — gentle technique throughout, no aggressive preparation, careful documentation, and referral if any new signs are progressing. See the professional considerations section above for the full assessment framework.
Frequently Asked Questions
Is nail lichen planus contagious?
No. Lichen planus is an autoimmune inflammatory condition and is not contagious. It cannot be passed between people through skin contact, shared tools, or any other route.
Can nail lichen planus be treated?
Yes. Treatment options include topical and intralesional corticosteroids, systemic anti-inflammatory agents, and other medications depending on severity. Treatment is most effective when initiated early, before significant scarring of the matrix has occurred. All treatment is managed by a dermatologist.
Can the nail grow back after lichen planus?
It depends on the extent of matrix scarring. If the matrix has been permanently scarred, the nail plate it would have produced is irreversibly lost and will not regrow. In cases where scarring is limited and treatment is effective, partial or complete recovery of nail growth is possible. This is why early treatment matters — the goal is to halt the inflammatory damage before irreversible scarring occurs.
How does nail lichen planus differ from nail psoriasis?
Both conditions can affect the nail matrix and produce structural changes. Key features that may help distinguish them include: pterygium unguis is characteristic of lichen planus and does not occur in psoriasis; the salmon patch and oil drop sign are characteristic of psoriasis and are not typically seen in lichen planus; and nail pitting — while common in psoriasis — is not a primary feature of lichen planus. Definitive differentiation requires clinical assessment and sometimes a nail biopsy.
Related Library Pages
Nail Conditions
Nail Anatomy
Some linked pages are currently in development and will be published progressively.
Professional Disclaimer
The information on this page is provided for educational purposes and is intended to support the professional knowledge of nail technicians and nail educators. It does not constitute medical advice. Any client presenting with progressive nail thinning, longitudinal ridging, pterygium formation, or any unexplained nail change should be referred to a qualified medical professional for assessment without delay.

About the Author
Radina Ignatova
Professional Nail Expert since 2014 | International Nail Educator | Founder of TheNailWiki and Artistic Touch Nail Training Academy
Radina Ignatova is a Professional Nail Expert since 2014 and an International Nail Educator specialising in dual forms, gel systems, polygel application, advanced nail structure, E-File techniques and professional salon safety.
She founded TheNailWiki to provide clear, safety-led nail education accessible to everyone, and Artistic Touch Nail Training Academy to deliver structured professional online nail courses.
Her teaching philosophy is centred on honest education — demonstrating real salon challenges, practical corrections and performance-based techniques rather than presenting only polished results.
Based in Scotland, UK, Radina contributes to advancing professional standards within the nail industry through structured educational resources and technical training.
Read full bio →About TheNailWiki
TheNailWiki is an independent educational platform dedicated to providing accurate, safety-led and professionally informed nail care information to professionals and enthusiasts worldwide. All content is created by qualified nail industry professionals and reviewed for technical accuracy.
For structured professional training, advanced masterclasses, and specialist technique courses, visit Artistic Touch Nail Training Academy.
This library page is published by TheNailWiki — an independent nail education resource maintained by nail industry professionals. Content is safety-led and professionally informed.